


The Big Prostate Problem
4 Cutting-Edge Solutions for Significant Enlargement

Hello, Health Enthusiasts!
Welcome to this week’s installment of our Informative Health Blog, lovingly written by yours truly every Saturday morning for the past decade (yes, I am that committed—or maybe just stubborn). These posts are my attempt to keep you informed, entertained, and hopefully learning something new! If health blogs aren’t your thing, you can easily opt out (I promise, no hard feelings). But if there’s a topic you’d love to see covered, drop me a line—I’m always open to suggestions (within reason, of course).
Now for some important news that really needs your attention!
Our new office is amazing, but… DO NOT GO TO THE MAYWOOD OFFICE!
Yes, I know, habits die hard. But seriously, if you show up at the old Maywood office, you’ll find a whole lot of nothing. Since late September, we’ve been in our shiny, lovely new space at 17-17 Route 208 North, Fair Lawn (just after the Fair Lawn Promenade). Google Maps and Waze might try to lead you astray—don’t let them. Your best bet? Tell your GPS to take you to “Summit Health, Fair Lawn Hub, NJ.”
A few pro tips for a smooth arrival:
· Our building comes up really fast and the sign for the building is small so keep those eagle eyes on alert.
· Parking is in the back of the building (not the Route 208 side).
· Enter from the back of the building, then head up to the second floor—SUITE 290 IS IN THE NORTHWEST CORNER OF THE BUILDING.
We know it’s a bit of a treasure hunt, but trust me, the prize is worth it! Thanks for sticking with us through this transition—we can’t wait to see you in our cozy new space.
I have advice from two patients regarding finding your way to the new office:
“I find it easier to use 18-01 Pollitt Drive, Fair Lawn on my GPS, which is Retro Fitness and is opposite your parking lot/entrance.”
“Fly from NJ to Zimbabwe, take a train to Egypt, go by boat to Hong Kong, then fly to NJ. Once there, go to your Teaneck office.”
Stay healthy, stay curious, and as always, thanks for reading!
FYI, On Thursday 12/19 I underwent a bilateral robotic-assisted, laparoscopic inguinal hernia repair at Hackensack Medical Center. My experience there was excellent and I am trying to be a good patient (photo showing me using incentive spirometer) and I have next week off to recuperate. It’s going to be tough for me to be sedentary for a few weeks. One thing is for sure…when it comes to surgery, I would rather be on the giving end than the receiving end! I’m feeling better this morning, but yesterday I felt like I was in the ring with Joe Frazier and he unleashed his fury on my abdomen.
Warm regards and happy holidays,
Andrew Siegel MD

The Big Prostate Problem: 4 Cutting-Edge Solutions for Significant Enlargement
When you're a spry 20-something, your prostate is a mere walnut-sized gland weighing in at a modest 15–20 grams. But fast forward a few decades, and that once-humble walnut can turn into something more akin to a Florida navel orange. Thanks to the combined forces of aging, testosterone, and genetics, many men experience prostate enlargement (a.k.a. benign prostatic hyperplasia, or BPH) starting around age 40. By some loose logic, a man’s age in years can sometimes mirror the size of his prostate in grams—though don’t take that rule to the bank!
As the prostate grows, it may squeeze the urethra (the tube that carries urine out of the bladder), leading to an assortment of unwelcome urinary symptoms. But here’s the kicker: prostate size doesn’t always match symptom severity. Some guys with small prostates suffer immensely, while others with monster-sized ones barely notice a thing. What really matters is the relationship between the growing gland and the prostatic urethra.
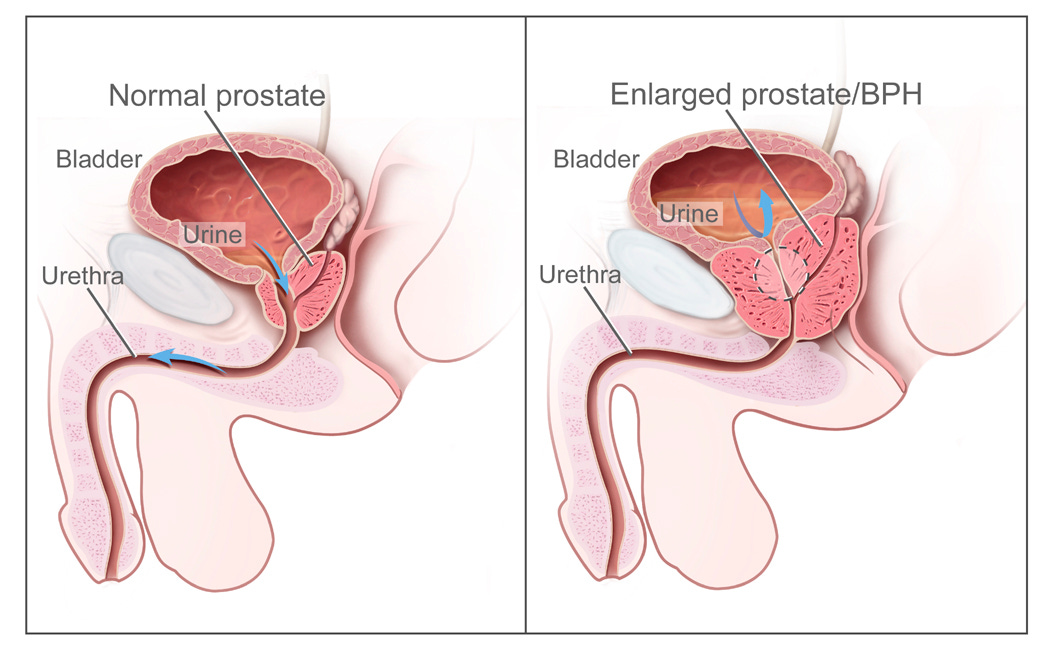
Attribution: National Cancer Institute, AV Number: CDR462221, Public domain, via Wikimedia Commons
In severe cases, an oversized prostate can block bladder emptying and lead to serious issues like the inability to urinate, bladder stones, urinary infections, kidney problems, or even full-on kidney failure. If medications don’t cut it, more invasive solutions come into play. Let’s dive into four innovative treatments that can tackle a significantly enlarged prostate: Robotic-Assisted Laparoscopic Simple Prostatectomy (RASP), Aquablation, Holmium Laser Enucleation of the Prostate (HoLEP), and Prostate Arterial Embolization (PAE).
Robotic-Assisted Laparoscopic Simple Prostatectomy (RASP)
Think of the traditional "simple prostatectomy" as scooping the fruit out of an orange while leaving the rind intact. In this case, the “fruit” is the benign overgrowth that’s causing the blockage, and the “rind” is the compressed outer layer of the prostate. While this used to require a big abdominal incision, modern robotic technology has made the procedure far less invasive.
Here’s how RASP works:
Tiny “keyhole” incisions are made instead of one large cut.
A high-definition camera and robotic tools are used to remove the obstructing tissue with extreme precision.
One surgeon controls the robotic system from a console, making micro-movements with joysticks, while another surgeon assists at the patient’s side. The result? Tremor-free precision and less surgeon fatigue (bonus points for the comfy chair at the console!).
The procedure is performed under anesthesia and typically requires an overnight hospital stay and a catheter for about one week. Recovery is relatively smooth, and the results—better urine flow and fewer symptoms—last for many years, especially for men with very large prostates.
Aquablation: The Waterjet Wonder
What if you could blast away excess prostate tissue with a high-powered waterjet? Enter Aquablation, a high-tech, minimally invasive option that combines imaging, robotics, and waterpower to treat enlarged prostates.
Here’s the scoop:
Your prostate is mapped out in 3D detail using a combination of ultrasound and cystoscopy.
A robotic-controlled waterjet (think pressure washer but way cooler) is used to precisely target and remove the overgrown tissue without heat damage.
A special instrument (resectoscope) is placed to trim out (resect) fluffy tissue of the bladder neck region and to visualize and cauterize bleeding.
The whole process is rapid and highly accurate, with minimal risk of side effects like erectile dysfunction or incontinence.
The procedure is performed under anesthesia and typically requires an overnight hospital stay and a catheter for at least several days.
Holmium Laser Enucleation of the Prostate (HoLEP): The Laser-Precision Fix
When it comes to dealing with an oversized prostate, HoLEP is like the Jedi Master of the bunch—laser-focused, minimally invasive, and effective. No messy incisions here—just a tiny scope and some high-tech laser magic.
Here’s the rundown on how HoLEP works:
A thin scope is inserted through the urethra (don’t worry, no scalpel involved). Once inside, a laser is used to precisely “enucleate” (or peel away) the inner tissue of the prostate, just like hollowing out the juicy part of an orange while leaving the tough peel intact.
Once the inner prostate tissue is freed, it’s minced into tiny, manageable bits by a device called a morcellator—think of it as a high-tech food processor. Those bits are then easily removed, so no need to worry about them getting passed through your urine.
Since HoLEP is performed through the urethra, there’s no need for any external incisions or stitches. The procedure is done under anesthesia, with a typical hospital stay of one night or so and a catheter for about a week.
This technique offers precision with minimal risk of complications like erectile dysfunction or incontinence. And since it clears out a significant amount of tissue, it often provides long-lasting relief.
Prostate Arterial Embolization (PAE): Starving the Beast
For men who aren’t candidates for traditional surgery, PAE offers a minimally invasive alternative. Instead of cutting, ablating, or enucleating, this procedure involves shrinking the prostate by blocking its blood supply.
Here’s how it’s done:
An interventional radiologist inserts a catheter into the femoral artery and carefully guides it to the tiny arteries feeding the prostate.
Micro-particles are injected to block blood flow, causing parts of the prostate to shrink and relieve urinary symptoms.
A catheter is left in place for an extended interval to allow the prostate to heal up.
PAE is an option for older men or those with health conditions that make general anesthesia or surgery risky. However, results can be hit or miss, as symptom relief doesn’t always correlate with the amount of prostate shrinkage. Side effects of PAE include urethral burning, fever, nausea and vomiting, and perineal pain from prostate ischemia (damage to the blood supply), short-term inability to urinate as well as the radiation exposure necessary to perform the procedure. PAE often involves an extended catheterization prior to resumption of spontaneous urinating.
Bottom Line: Dealing with an oversized prostate doesn’t have to mean resigning yourself to annoying symptoms. Whether you’re considering the robotic precision of RASP, the high-tech waterjet of Aquablation, the laser precision of the HoLEP, or the blood flow-blocking power of PAE, today’s options are more effective—and less intimidating—than ever before. So, if you’re feeling the squeeze, rest assured that innovative solutions are within reach!
Wishing you the best of health and happy holidays,
Andrew Siegel, MD
Very helpful and informative updates. A companion blog on pros & cons on each of these procedures would be useful. Wishing you a speedy recovery. Happy Holidays.