


Understanding UPJ (Ureteropelvic Junction) Obstruction
Key Insights

Greetings, seekers of medical wisdom. Today we delve into the intricacies of UPJ (Ureteropelvic Junction) obstruction, a topic worthy of our attention. This entry was prompted by me consulting on a run of patients with UPJ obstruction over the course of a short period of time, many more than typically expected to be seen as the occurrence of this type of obstruction is relatively rare.

(Image above: Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. - Own workDecoding UPJ: A Crucial Anatomical Crossroad)
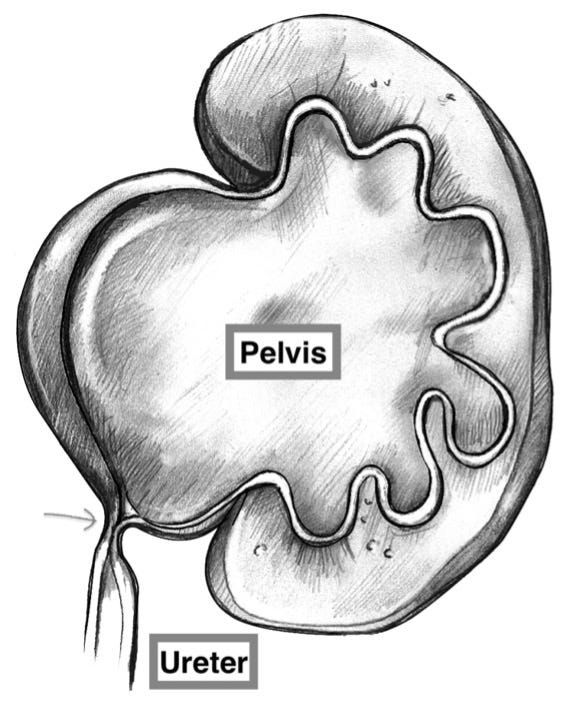
The UPJ is the junction where the kidney's internal urine collection chamber (the pelvis) converges with the tubular structure draining urine to the bladder (the ureter). The image above shows the normal anatomy of the kidney. Note the smooth transition of the renal pelvis into the ureter.
UPJ obstruction? It's akin to a “roadblock” that hinders the smooth flow of urine that can result in quite a “traffic backup." See drawing below:
UPJ Demographics
UPJ obstruction occurs in about 1 in 1500 people in the United States, is more common in males than females and more commonly involves the left kidney than the right kidney. 10% of cases involve both kidneys.
Silent Predicament: Asymptomatic Encounters
A notable fraction of adults harboring UPJ obstruction have no symptoms whatsoever. This condition often unveils itself incidentally during diagnostic scans aimed at addressing unrelated medical concerns. Swelling of the kidney pelvis, aka hydronephrosis (hydro = water, nephrosis = kidney), becomes the unexpected finding.
Note: For many, UPJ obstruction is stealthy, revealing itself only under the lens of medical imaging.
Early Onset Challenges: Infancy and Beyond
UPJ obstruction sometimes makes its debut during fetal development, visible on prenatal ultrasounds. In infancy, significant cases may manifest as febrile urinary tract infections or the presence of an abdominal mass. However, the revelation may be deferred until childhood or adulthood, marked by symptoms such as blood in urine, flank pain, nausea, and vomiting.
Underlying Factors: A Spectrum of Causes
Whether congenital (present at birth) or acquired (developed some time after birth), UPJ obstruction stems from either intrinsic or extrinsic factors. Intrinsic contributors include scar tissue, malfunctioning segments of the ureter, ureteral kinks, high ureteral insertion into the renal pelvis, or stones lodged in UPJ. Extrinsic factors often involve blood vessels obstructing the path of the ureter or external scar tissue, aka retroperitoneal fibrosis.
Dietl's Crisis: An Ominous Symptom
Dietl's crisis is episodic, crampy upper abdominal pain, nausea, and vomiting, signifying intermittent UPJ obstruction. The cause is acute hydronephrosis, often induced by an anomalous renal blood vessel at the lower kidney pole constricting the pelvis, but it can also be due to intrinsic causes.
Note: Interestingly, UPJ obstruction cases are not uncommonly revealed in college students, with Dietl's crisis triggered by excessive beer consumption at fraternity parties!
Long-term Ramifications: Kidney Functionality at Stake
Persistent UPJ obstruction may inflict substantial harm on kidney function. The swelling and increased pressure within the kidney pelvis due to the obstruction may lead to atrophy over time, impacting the organ's functionality.
Diagnostic Odyssey: Navigating Imaging Modalities
Evaluating UPJ obstruction entails a comprehensive analysis of kidney anatomy and function. This is achieved through non-invasive imaging methods such as ultrasound, CT (computerized tomography), or MRI (magnetic resonance imaging). Renal scans, incorporating diuretic administration (use of a medication that induces the kidneys to produce a lot of urine) to provoke obstruction, contribute crucial insights into kidney function. This functional scan will provide quantitative information about how much each kidney is contributing to total renal function and will help determine whether or not intervention is necessary.
Strategic Response: To Intervene or Not?
In asymptomatic cases with unimpaired kidney function, a watchful waiting approach suffices. Conversely, when symptoms are present or compromised function of the kidney is apparent, surgical intervention becomes imperative. A robotic-assisted, laparoscopic procedure, aka pyeloplasty, is a highly effective means of repairing a UPJ obstruction. This typically involves surgical excision of the obstructed segment followed by reconstruction of the UPJ to allow for the unobstructed flow of urine from kidney to bladder. If the UPJ obstruction is due to an extrinsic compression from a crossing blood vessel, the ureter is detached from the renal pelvis and rerouted around the crossing blood vessel.
Wishing you the best of health and a wonderful holiday weekend,
Andrew Siegel MD
Interesting article. Wasn’t aware of this condition.